Get your free personalized podcast brief
We scan new podcasts and send you the top 5 insights daily.
The SmallTap cradle was conceived when a frustrated hospitalist, after a difficult procedure, had a chance encounter with a neonatologist who was also a former architect and teaching a device design class. This fusion of acute clinical need with outside expertise sparked the innovation.
Related Insights
The core innovation for the Cobra OS wasn't a complex discovery but the disciplined application of a known principle: miniaturizing endovascular devices always makes them safer. By focusing on shrinking the device, they inherently improved safety by reducing the size of the arterial access site.
The transition from academia to entrepreneurship is most successful when the focus shifts from pure science or technology to solving a tangible, pre-existing clinical problem. This ensures market interest, clinical adoption, and ultimately, patient impact from the outset.
The solution to a high-tech problem like concussions was sparked by observing an old Mark V Navy dive helmet in a restaurant. This shows that innovative concepts don't always come from the cutting edge. They can emerge from re-interpreting the core principles of historical artifacts and applying them to modern challenges.

Successful MedTech innovation starts by identifying a pressing, real-world clinical problem and then developing a solution. This 'problem-first' approach is more effective than creating a technology and searching for an application, a common pitfall for founders with academic backgrounds.
The next wave of MedTech innovation won't just come from engineers. It will come from creating tools that allow surgeons and clinicians—those who see problems firsthand—to easily prototype and de-risk new device concepts, vastly expanding the market for innovation itself.
The most critical role for a physician co-founder extends beyond the initial idea. They must act as the primary evangelist and validator, sharing the engineering progress with their peers to ensure the device's design and function align with the broader clinical community's needs and vision.
The idea for a living computer came not from biologists, but from engineers with backgrounds in signal processing. This highlights how breakthrough innovations often occur at the intersection of disciplines, where outsiders can reframe a problem from a fresh perspective.

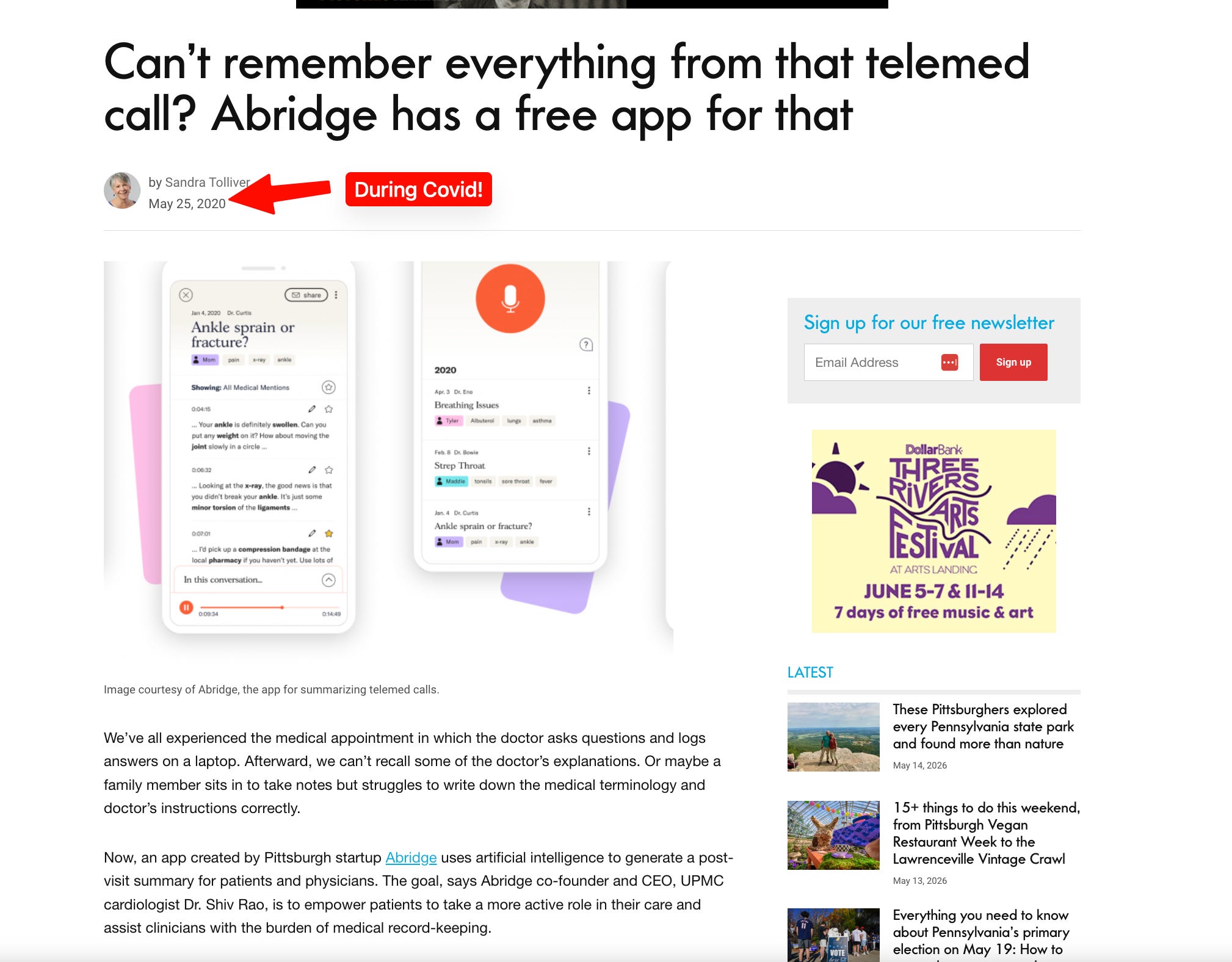
Abridge's secret weapon for building clinically relevant products is the "clinician scientist" role. These are team members with clinical backgrounds (e.g., MDs) who are also deeply technical. By embedding them in product teams, the company ensures that clinical usefulness and safety are baked into development and evaluation from day one.
Large medical device companies have rigid innovation cycles that may not align with a clinician's new idea. Dr. Adam Power discovered that to ensure his invention would actually reach patients, he had to commercialize it himself rather than waiting for a large company's timeline.
For clinicians turned entrepreneurs, the first step is not ideating a solution. It's rigorously studying a problem they face, quantifying it, and confirming it's a universal issue across many institutions. True innovation stems from this deep, problem-first validation, not from a technology-first approach.